|
|
|
Free Neuropathology 2:23 (2021) |
|
Case Report |
|
Hydrophilic polymer embolism identified in brain tumor specimens following Wada testing: A report of 2 cases |
|
Vanessa S. Goodwill MD*1, Michael G. Brandel MD, MAS*2, Jeffrey A. Steinberg MD2, Thomas L. Beaumont MD, PhD2, Lawrence A. Hansen MD1 |
|
1 Department of Pathology, University of California, San Diego, USA |
|
Corresponding author: |
|
Submitted: 28 July 2021 Accepted: 28 August 2021 Copyedited by: Deborah McIntyre Published: 2 September 2021 |
|
Keywords: Embolism, Vascular access devices, Brain infarction, Glioma, Vasculitis |
|
Abstract Hydrophilic polymers are commonly used as coatings on intravascular medical devices. As intravascular procedures continue to increase in frequency, the risk of embolization of this material throughout the body has become evident. These emboli may be discovered incidentally but can result in serious complications including death. Here, we report the first two cases of hydrophilic polymer embolism (HPE) identified on brain tumor resection following Wada testing. One patient experienced multifocal vascular complications and diffuse cerebral edema, while the other had an uneventful postoperative course. Wada testing is frequently performed during preoperative planning prior to epilepsy surgery or the resection of tumors in eloquent brain regions. These cases demonstrate the need for increased recognition of this histologic finding to enable further correlation with clinical outcomes. Introduction Intravascular devices, such as catheters, guidewires, and stents are commonly coated with hydrophilic polymer material. This hydrophilic polymer material has significant procedural benefits, such as acting as a lubricant to decrease vascular trauma, and reducing vascular spasm.1 Over the past several decades there has been a drastic increase in the prevalence of minimally invasive endovascular medical procedures. As a result, there has been growing recognition of the risk of embolization of hydrophilic polymer coating material throughout the body.2,3 Wada tests (also known as intracarotid sodium amobarbital procedure, ISAP) are commonly performed before ablative procedures or resections for epilepsy or tumor to assess hemispheric dominance for language. There is a low risk of complications following Wada testing including seizures, status-epilepticus, vascular spasm, and transient encephalopathy.4 Hydrophilic polymer emboli, however, have not previously been reported following pre-operative Wada testing. Here, we describe two patients who underwent primary brain tumor resection following Wada testing. In both resection specimens, intravascular hydrophilic polymer material with associated foreign body giant cell reaction was identified, and in one case there was evidence of associated acute ischemic change in surrounding neurons. To our knowledge, the current work represents the first report of this histologic finding after Wada testing. Case Summaries Case 1 Clinical Findings: A 55-year-old right-handed man presented with new-onset generalized tonic-clonic seizures. Magnetic resonance imaging (MRI) revealed a non-enhancing infiltrative and expansile T2-hyperintense mass centered within the right superior temporal gyrus (Fig. 1a-b). The patient underwent bilateral Wada testing. Vascular access was obtained via the right femoral artery using the modified Seldinger technique. A 5-French angled glide diagnostic catheter was introduced over a 0.035 Terumo Glidewire into the descending thoracic aorta and then the cervical internal carotid artery under direct fluoroscopic visualization. A Codman Prowler Select Plus infusion microcatheter with a Synchro 2 microwire was used to catheterize the internal carotid artery just distal to the posterior communicating artery. An angiographic run was performed to confirm catheter position prior to Brevital (methohexitol) infusion (Fig. 1c). The Wada test demonstrated clear left hemisphere language dominance and greater left hemisphere memory support.
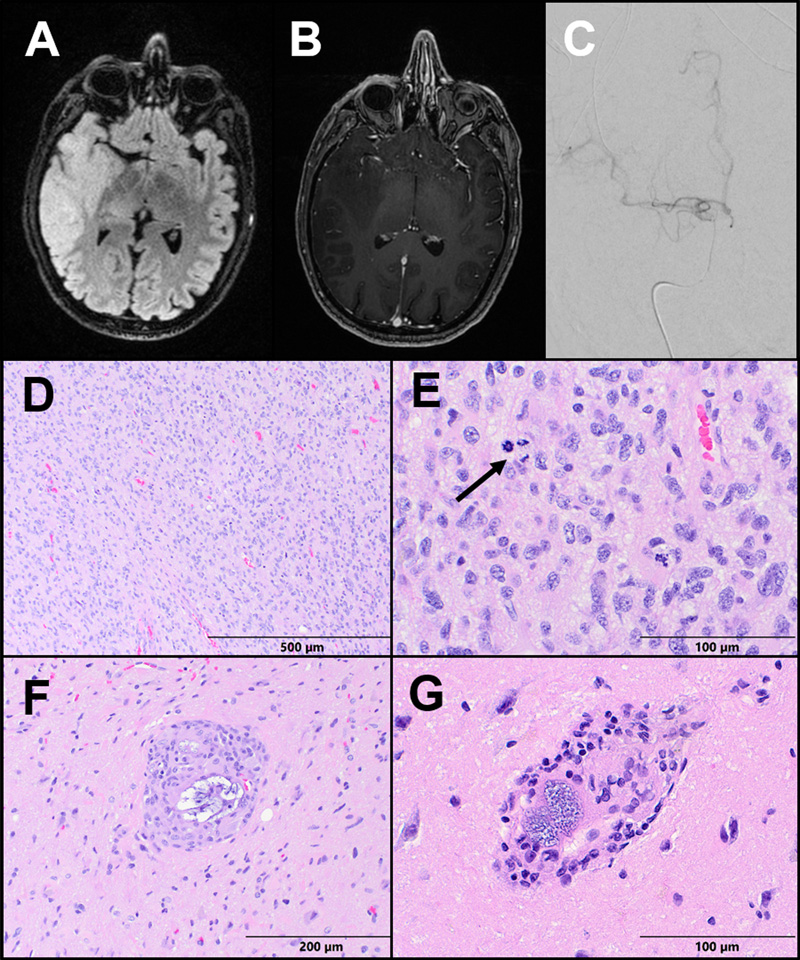
Figure 1: Case 1 Imaging and Pathology. (A) Axial T2-FLAIR and (B) T1 post-contrast sequences of a brain MRI demonstrating a non-enhancing infiltrative and expansile T2-hyperintense mass centered within the right superior temporal gyrus. (C) A PA view of digital subtraction angiogram demonstrating a microcatheter within the right internal carotid artery. (D-E) The tumor resection demonstrates a moderately to highly cellular infiltrating glioma, with significant nuclear atypia and scattered mitoses (arrow). (F-G) Parenchymal vessels within the resection display giant cell vasculitis and contain basophilic granular foreign material consistent with hydrophilic polymer. Five weeks later, the patient underwent a right temporo-parieto-occipital craniotomy for tumor resection. His postoperative course was complicated by a seizure upon awakening with right frontal venous infarct and layering remote cerebellar hemorrhage. He experienced weakness in his left upper and lower extremities and was discharged to a rehabilitation facility with antiepileptic and steroid medications. At 5 months follow-up, the patient had recovered his motor function with no additional seizures, was able to walk over a mile per day without assistance and was tolerating adjuvant chemoradiation. Subsequently, post-treatment MRIs demonstrated a heterogeneously enhancing, centrally necrotic mass in the right temporo-parietal tumor bed with no associated hyperperfusion, characteristic of evolving pseudoprogression. These findings were associated with marked hemispheric cerebral edema refractory to steroid treatment and requiring bevacizumab (Fig. 2).
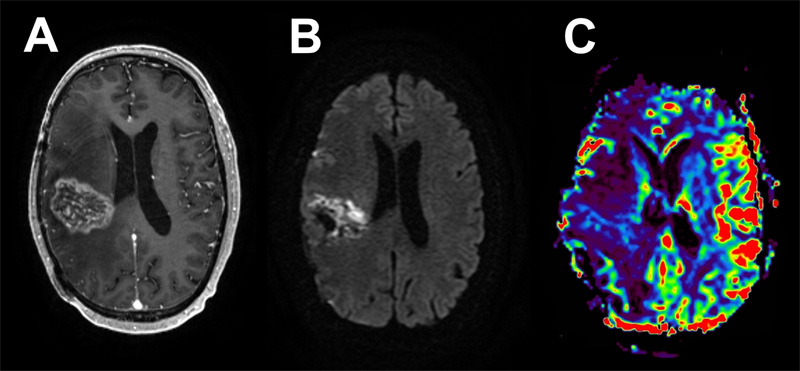
Figure 2: Case 1 Post-treatment imaging findings. An 8-month post-operative MRI following chemo-radiation showed evidence of pseudoprogression with significant associated cerebral edema. Axial T1 post-contrast (A) shows a heterogeneously enhancing, centrally necrotic mass, with restricted diffusion on DWI (B), and no associated hyperperfusion (C). Pathology: Evaluation of the primary resection specimen revealed a moderately to highly cellular diffusely infiltrating glioma. There was significant pleomorphism and focally frequent mitoses, but no microvascular proliferation or necrosis, meeting histologic criteria for anaplastic astrocytoma, WHO Grade III (Fig. 1d-e). Molecular analysis by next-generation sequencing (NGS) and microarray revealed features of primary IDH-wildtype glioblastoma, including EGFR amplification, and the tumor was upgraded to WHO Grade IV.5 Additionally noted on pathologic examination were scattered foci of giant cell vasculitis and intravascular foreign material. The foreign material was granular, blue-gray and non-polarizable, morphologically consistent with hydrophilic polymer material. No surrounding ischemic changes were identified (Fig. 1f-g). Case 2 Clinical Findings: A 24-year-old right-handed female with no significant past-medical history presented after suffering a generalized tonic-clonic seizure at work. MRI showed a large, non-enhancing infiltrative T2 hyperintense mass centered in the right hippocampus and inferior temporal lobe with regional mass effect (Fig. 3a-b). She underwent stereotactic biopsy at an outside facility, which demonstrated a WHO Grade II diffuse astrocytoma.
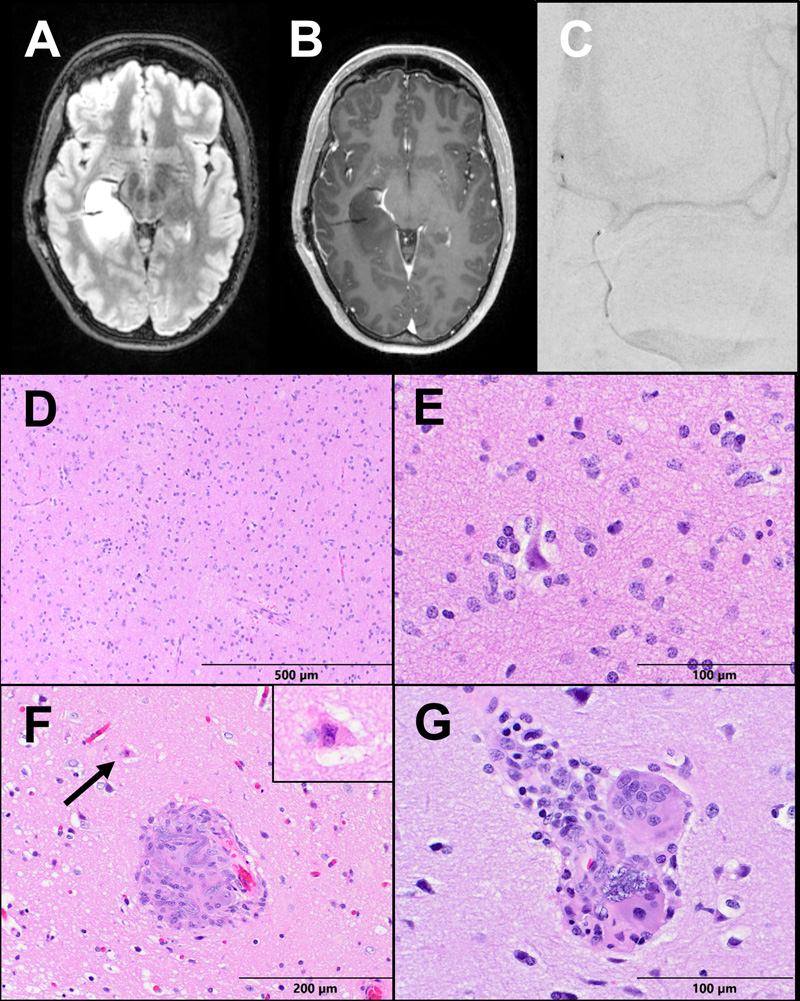
Figure 3: Case 2 Imaging and Pathology. (A) Axial T2-FLAIR and (B) T1 post-contrast MRI brain sequences demonstrate a non-enhancing infiltrative T2 hyperintense mass centered in the right hippocampus and inferior temporal lobe. (C) PA view of a digital subtraction angiogram demonstrates a microcatheter within the left internal carotid artery. (D) The tumor resection shows a moderately cellular glioma infiltrating white matter and (E) cortex with perineuronal satellitosis. (F) A hypereosinophilic ischemic neuron (arrow and inset) is seen next to a vessel occluded by hydrophilic polymer material with associated inflammation. (G) Some vessels contain multinucleate foreign-body giant cells consuming basophilic polymer material. The patient underwent bilateral Wada testing with the same microcatheterization technique described in Case 1 (Fig. 3c). Injections of both sodium methohexital (Brevital) and amobarbitol (Amytal) were completed, and language representation was identified in the left hemisphere. Three weeks later, the patient underwent right frontotemporal craniotomy for tumor resection. She had an uncomplicated postoperative course and was discharged home on postoperative day 3 at her baseline functional status, with no neurologic deficits. She remains neurologically intact and seizure-free 9 months postoperatively. Pathology: Histologic examination of the resection specimen showed a paucicellular infiltrating glioma composed of atypical astrocytes with enlarged, irregular, and hyperchromatic nuclei. No mitoses, necrosis, or microvascular proliferation were detected (Fig. 3d-e). NGS was performed and an IDH1-R132H mutation was identified, along with mutations in TP53, and ATRX. The final diagnosis was diffuse astrocytoma, IDH-mutant, WHO Grade II. Also noted multifocally were a few small parenchymal vessels containing non-polarizable granular blue-gray foreign material consistent with HPE. Surrounding these vessels was foreign-body giant cell reaction, and a few hyper-eosinophilic acutely ischemic neurons (Fig. 3f-g). Discussion Hydrophilic polymer embolization in cerebral vessels was first reported in 1997 by Barnwell et al. in four cases involving use of a microcatheter with hydrophilic coating for cerebral angiography (three autopsy specimens after endovascular thrombolysis for acute ischemic stroke, and one biopsy specimen of a previously-embolized meningioma).6 Emboli were described as basophilic and granular, identical in histologic appearance to hydrophilic polymer material seen on sections of microcatheter submitted for histologic analysis. HPE have since been identified widely throughout the body, including the lungs, skin, heart, and central nervous system (CNS).3,7–11 HPE may be discovered incidentally or in association with a wide range of complications. Reported sequelae of HPE throughout the body include vasculitis, thrombosis, infarction, and even death.12 Additionally, there is a significant range in the time-course of presentation and duration, spanning acute, subacute, and delayed symptomatology. One study described evidence of persistent inflammation over three years after the intravascular procedure.13 HPE has been reported following various neuro-interventional procedures such as aneurysm coil embolization, aneurysm flow diversion, intra-arterial thrombolysis, and diagnostic cerebral angiography, and may result in a variety of CNS complications.12,14,15 Mehta et al. reported a series of 32 cases of HPE within the CNS, with findings including vasculitis, granuloma formation, chemical meningitis, ischemia, and hemorrhage.8 These findings were associated with a 38% incidence of stroke and 28% rate of death. The high rate of morbidity and mortality secondary to HPE in this study, however, may be an overestimate as patients were identified in part by their adverse clinical outcome, and types of catheterization also included central venous access and hemodialysis catheterization. Here, we report two cases of HPE identified in brain tumor resection following pre-operative Wada testing. To perform a Wada test, sodium methohexital (Brevital) or amobarbital (Amytal) is injected into right or left internal carotid artery, which results in ipsilateral hemispheric anesthetization. At our institution, a Neuropsychologist conducts a baseline evaluation prior to Wada testing, and then repeats this assessment during injections of each hemisphere. In addition, an Epileptologist interprets the continuous EEG and compares background activity in each hemisphere to activity during injection to confirm appropriate post-anesthetic changes. A variety of microcatheters are utilized at our institution, including the Prowler Select Plus which is a braid/coil microcatheter with a radiopaque tip and hydrophilic coating. To our knowledge, no prior reports have described an association between this microcatheter and HPE. The rate of complications following cerebral angiography is between 0.3-1.3%, and only a fraction of these are neurologic complications with lasting effects.16,17 The complication rate for Wada testing is likely around 2%, although some studies have reported up to 10%.4 Of particular interest, our patient from Case 1 suffered immediate post-craniotomy vascular complications possibly induced or exacerbated by HPE-associated vasculitis and thrombosis, although there were no immediate or delayed complications from the Wada test on its own. Although this patient had recovery of neurological function and was ambulatory and independent with activities of daily living, he had early radiologic evidence of pseudoprogression complicated by cerebral edema refractory to steroid treatment and requiring bevacizumab. Though one can only speculate, as no additional tissue resection was performed following chemo-radiation, it is possible HPE associated vascular changes in this patient may have also contributed to his significant refractory cerebral edema and extent of pseudoprogression. The patient from Case 2 has suffered no adverse clinical sequela to date despite histologic evidence of vasculitis and surrounding acute ischemia. HPE-induced vasculitis and thrombosis may contribute to surgical and post-operative vascular complications in patients undergoing craniotomy for tumor resection or during epilepsy surgery. As the clinical sequelae of hydrophilic polymer emboli can be quite severe based on the findings of several case series,8,12 clinicians and surgeons should be made aware of their presence when identified histologically. Therefore, we recommend including the presence of HPE and any associated vascular or ischemic changes as a separate diagnostic line in pathology reports when identified in biopsy or resection specimens to allow for clinical correlation in the event of any unforeseen vascular complications (See example below, Case 2). Right temporal brain mass, resection:
COMMENT: Hydrophilic polymers are applied as surface coatings on vascular devices, and embolization of this material has been reported following various vascular procedures. Hydrophilic polymer emboli may be an incidental finding, but can also result in a range of vascular complications. Clinical correlation is suggested. Furthermore, the incidence of HPE following neuro-interventional procedures is likely under-recognized. Published studies are limited by selection bias; however, and neither the overall rate of HPE after cerebral angiography nor the true rate of clinical complications in the setting of cerebral HPE can be identified from the current literature. As such, it is important to recognize HPE histologically so that prospective clinical outcome studies of patients undergoing neuroendovascular procedures prior to cerebral tissue biopsy may be performed. Disclosures The following authors have nothing to disclose: Vanessa S. Goodwill, Michael G. Brandel, Jeffrey A. Steinberg, Thomas L. Beaumont, Lawrence A. Hansen. References 1. Koga S, Ikeda S, Futagawa K, et al. The use of a hydrophilic-coated catheter during transradial cardiac catheterization is associated with a low incidence of radial artery spasm. Int J Cardiol. 2004;96(2). 2. Mehta RI, Mehta RI. Hydrophilic Polymer Embolism: An Update for Physicians. Am J Med. 2017;130(7). 3. Mehta RI, Mehta RI, Choi JM, Mukherjee A, Castellani RJ. Hydrophilic polymer embolism and associated vasculopathy of the lung: Prevalence in a retrospective autopsy study. Hum Pathol. 2015;46(2). 4. Beimer NJ, Buchtel HA, Glynn SM. One center’s experience with complications during the Wada test. Epilepsia. 2015;56(8). 5. Brat DJ, Aldape K, Colman H, et al. cIMPACT-NOW update 5: recommended grading criteria and terminologies for IDH-mutant astrocytomas. Acta Neuropathol. 2020;139(3). 6. Barnwell SL, D'Agostino AN, Shapiro SL, Nesbit GM, Kellogg JX. Foreign bodies in small arteries after use of an infusion microcatheter. AJNR Am J Neuroradiol. 1997 Nov-Dec;18(10):1886-9. 7. Komoda S, Ozawa H, Yuasa T. Hydrophilic polymer embolism in the lung as an adverse event: Autopsy case of thromboembolisms in multiple organs associated with heparin-induced thrombocytopenia. Circ J. 2018;82(2). 8. Mehta RI, Mehta RI. Polymer-induced central nervous system complications following vascular procedures: Spectrum of iatrogenic injuries and review of outcomes. Hum Pathol. 2016;53. 9. Mehta RI, Mehta RI. Hydrophilic Polymer Embolism: Implications for Manufacturing, Regulation, and Postmarket Surveillance of Coated Intravascular Medical Devices. J Patient Saf. 2018 Mar 19:10.1097 10. French B, Ranguelov R, Johansen K, Tan SL. Ischemic Toe Ulceration Due to Foreign Body Embolus From Hydrophilic Polymer-Coated Intravascular Device. Vasc Endovascular Surg. 2019 Oct;53(7):606-8. 11. Rosen LE, Singh RI, Mahon B. Myocardial hydrophilic polymer emboli following cardiac catheterization: A case report and literature review. Cardiovasc Pathol. 2014;23(3). 12. Mehta RI, Mehta RI, Solis OE, et al. Hydrophilic polymer emboli: An under-recognized iatrogenic cause of ischemia and infarct. Mod Pathol. 2010;23(7). 13. Sequeira A, Parimoo N, Wilson J, Traylor J, Bonsib S, Abreo K. Polymer embolization from minimally invasive interventions. Am J Kidney Dis. 2013;61(6). 14. Shapiro M, Ollenschleger MD, Baccin C, et al. Foreign body emboli following cerebrovascular interventions: Clinical, radiographic, and histopathologic features. Am J Neuroradiol. 2015;36(11). 15. Geisbush TR, Marks MP, Heit JJ. Cerebral foreign body reaction due to hydrophilic polymer embolization following aneurysm treatment by pipeline flow diversion device. Interv Neuroradiol. 2019;25(4). 16. Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G, Montanera W. Neurologic complications of cerebral angiography: Prospective analysis of 2,899 procedures and review of the literature. Radiology. 2003;227(2). 17. Fifi JT, Meyers PM, Lavine SD, et al. Complications of Modern Diagnostic Cerebral Angiography in an Academic Medical Center. J Vasc Interv Radiol. 2009;20(4).
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |