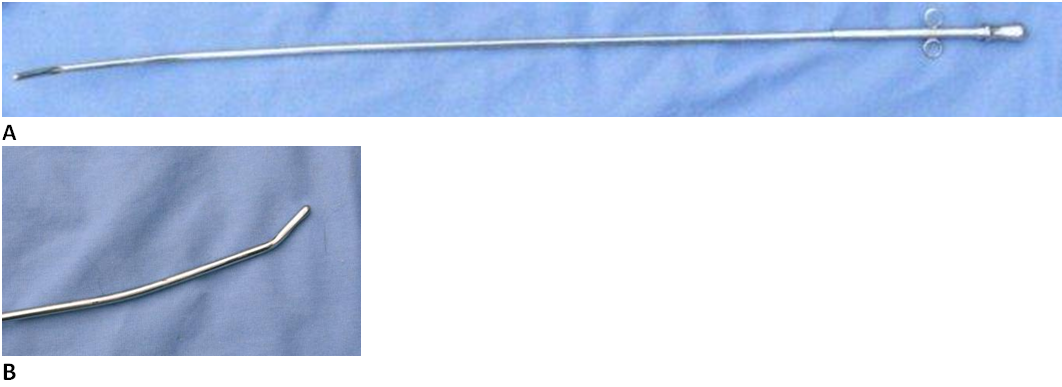
Figure 1: (A) The Nielson catheter that has been manually adapted to include a 30 degree distal bend at the tip and a 10 degree mid-shaft curve. (B) Shows a close up of the distal tip.
Use of a Reverse Thermodynamic Gel to Manage Chronic Shedding in Equine Strangles
Mark Bowen BVetMed MMedSci PhD CertVA CertEM(IntMed) DipACVIM-LAIM PFHEA FRCVS1*
1Oakham Veterinary Hospital, Ashwell Road, Oakham LE15 7QH
*Corresponding Author (Mark.Bowen@nottingham.ac.uk)
Vol 2, Issue 3 (2017)
Published: 24 Jul 2017
Reviewed by: Tim Mair (BVSc PhD DEIM DESTS DipECEIM AssocECVDI MRCVS) Kate McGovern (BVetMed CertEM(Int.Med) MS DACVIM DipECEIM MRCVS)
DOI: 10.18849/VE.V2I3.109
Strangles is a common condition in equine practice with high morbidity. Management of outbreaks is complicated by the development of asymptomatic carriers with the causative organism (Streptococcus equi var equi) being retained within the guttural pouch1,2. Treatment of carriers relies upon removal of physical infection and locally administered antimicrobials. Combinations of penicillin with gelatin has been recommended3 to prolong antimicrobial concentrations within the guttural pouch.. This involves the melting of gelatin, to allow mixing and infusion of the warm liquid. The horses head is raised for 20 minutes while the solution sets as it cools, preventing loss of solution. These steps are often difficult to achieve outside of a hospital environment.
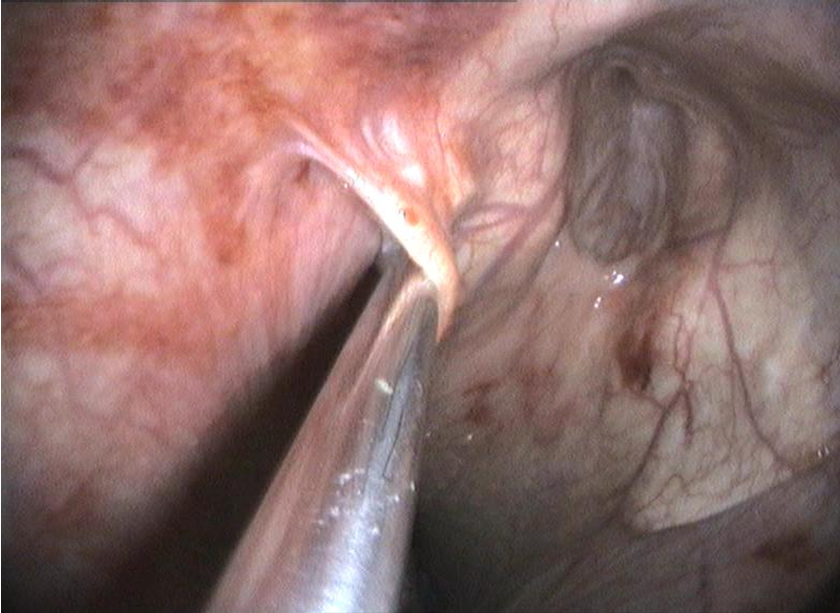
The availability of reverse thermodynamic agents, that are liquid when cool and solidify as they warm, have been used for local delivery of medicines when treating otitis externa in dogs. These create an opportunity to retain antibiotics in the guttural pouch without the complexity of melting gelatin in a field setting. Benzylpenicillin in poloxamer gel was specially formulated at a concentration of 120mg/ml in a 25ml solution by a commercial specials manufacturer (BOVA UK). An asymptomatic strangles carrier was identified based on PCR detection of bacterial DNA from a guttural pouch lavage. After sedation, a stainless steel uterine catheter (Nielson catheter) was adapted by manually placing a 30 degree bend at the distal 3cm tip of the catheter and approximately a 10 degree curve along the distal 15cms of the catheter (Figure 1). The catheter was placed along the ventral meatus with the tip angled ventrally. Once the catheter was in the pharynx, the tip was rotated ventrally and abaxially as the catheter was advanced into the guttural pouch; location was confirmed endoscopically (Figure 2). Cooled, pre-formulated poloxamer gel was infused through the urinary catheter and the catheter immediately removed. The head was maintained in a neutral position and a small amount of gel that exited the pouch as the catheter was removed, remained adherent to the pharyngeal wall demonstrating that it had already partially set.
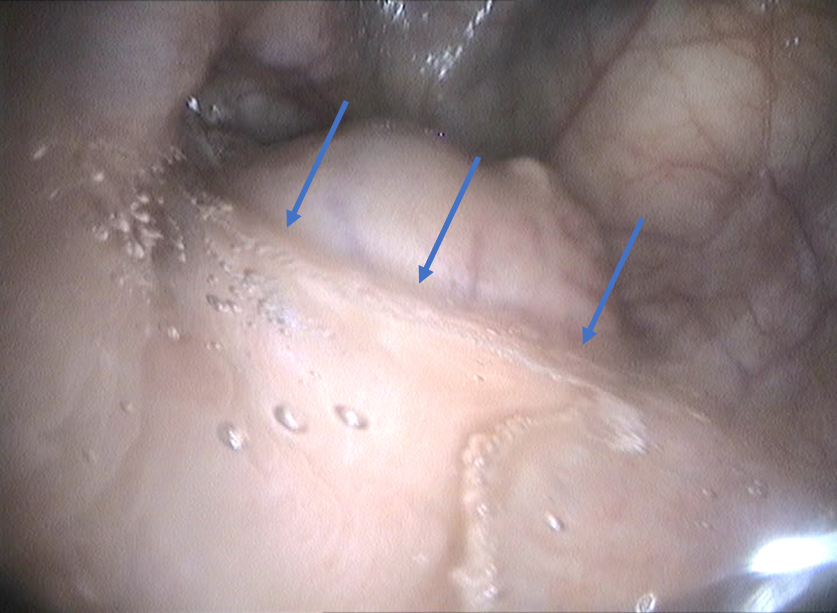
Endoscopic assessment of the guttural pouch immediately after the infusion demonstrated that the poloxamer gel had partially set within the floor of the medial compartment of the treated pouch (observed 4 minutes 25 seconds after infusion: Figure 3). Treatment was repeated on three consecutive days and cure was determined by three guttural pouch lavages taken at weekly intervals, starting one week after the last treatment. This confirms the value of locally infused antibiotics in the management of strangles carriers. The reverse thermodynamic poloxamer gel provided a practical method for retaining antibiotics within the pouch with the need for complex mixing or prolonged raising of the horses head. This will facilitate management of this frustrating condition in the field. Administration through an endoscopic catheter is not recommended since the poloxamer gel partially solidifies within the biopsy channel due to the heat from the light source.
This case highlights the value of specially formulated medicines in the management of complex diseases by providing novel delivery vehicles.
The author declares no conflict of interest.