Stefano Ricci
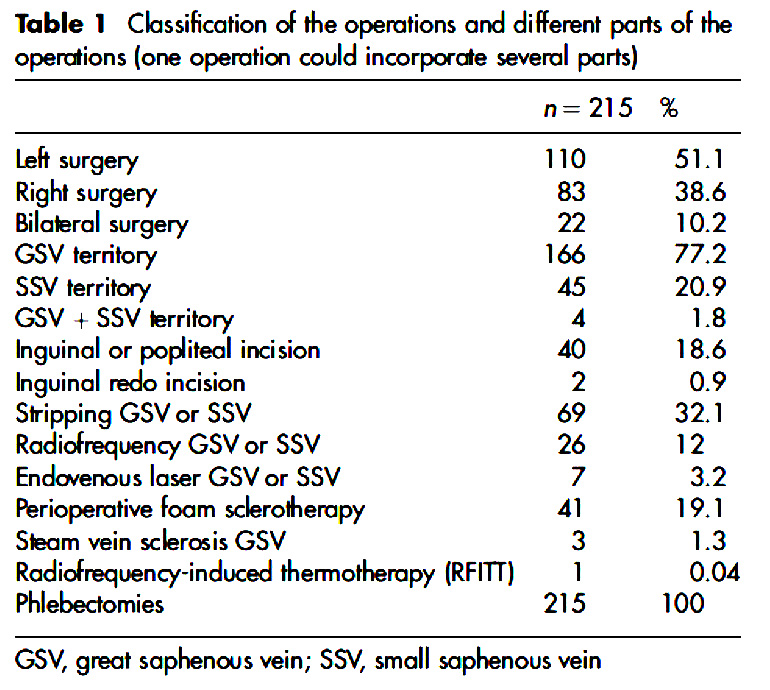
AbstractThe aim of this survey was to study the feasibility of varicose vein surgery under tumescent local anesthesia (TLA). A total of 215 patients at two private surgical centers in France were included. All the operations were performed under TLA without any intravenous sedation. The tumescent liquid was obtained by diluting lidocaine 1% (20 mL containing 200 mg lidocaine). A solution of 14 mL of 1% lidocaine (with 1:100,000 epinephrine) was diluted in a bottle with 500 mL of 1.4% sodium bicarbonate (lidocaine dilution at approx. 0.028%). Injections were performed with 25 gauge needles, with syringes or an electric pump. Patients had to arrive in the morning after eating breakfast as usual. Surgery was performed in an operating theater without any particular monitoring. The patients’ faces were not covered with sterile operative fields to allow visual and oral communication. Operations included either phlebectomies or stripping or thermoablation of truncular segments (Table 1). Double compression with a class II elastic stocking was placed for 48 h and then replaced with one single stocking for one week. Every patient filled in a questionnaire to evaluate the surgery-related pain on an analog scale ranging from 0 to 10, along with pain duration (from some seconds to some minutes or much longer). Patients could return home the day after surgery and they then filled in the same questionnaire again. The patients returned their questionnaire two months later at their postoperative check-up. The majority of the patients were classified C2 while 30 were classified C3, 26 were C4a, 4 were C4b, one was C5 and one was C6. Mean VCSS score was 1.5+1.4 (1.0-13.0). Complete phlebectomies were performed in all patients. Mean number of phlebectomies was 24.0+13.0 (3.0-63.0). Mean volume of tumescence was 268.1+127.1 mL. Mean dilution of lidocaine epinephrine in relation to patient mean weight (65.7+12.0 kg; range 42.0-106.0) was 75.1+35.6 mg of lidocaine and 0.037+0.0178 mg of epinephrine injected. This represents a mean 1.17+0.54 mg of lidocaine per kg bodyweight and 0.58+0.27 mg epinephrine/ kg bodyweight. The different levels of pain sustained during surgery (Figure 2) show that mean pain level was 2.7+2.1 (range 0.0-9.0). In 69.3% of cases, the pain was considered light (0–3), in 25.5%, moderate (4–6) and in 5.2% severe (7–10). In 91.9% of the cases, surgery was considered as not very or not at all painful. In 8.1% of the cases, surgery was considered to be rather painful; for 81.2% of these patients, pain lasted for only a few seconds and for 17.4% for some minutes. No patients considered their surgery to be extremely painful. In cases in which more than 30 incisions were performed, patients felt significantly more pain (3.4+2.1) than when 16-30 incisions (2.2+1.9) or less than 16 incisions (2.8+2.2) were performed. When asked whether they would undergo this type of anesthesia again, 97.7% of the patients said they would. Mean surgery time between the first TLA injection and the last phlebectomy was 32+14 min (8–77 min). In 82.8% of the cases, the patients were dismissed less than 2 h after surgery. Mean duration of the postoperative period was one hour and 45 min (range 30 min–7 h). Mean length of hospital stay was 4 h and 10 min (2–9 h). This operation with parenteral sedation carried out by an anesthesiologist would have cost 52,839 euros while surgery with tumescent local anesthesia cost 30,788 euros; a saving of 22,051euros. The use of pure sodium bicarbonate 1.4% as tumescent solution, instead of saline solution or Ringer’s solution, facilitates surgery by eliminating the onset time dilution. Furthermore, in this study, lidocaine dilution was 0.028% and epinephrine dilution was 0.14:1,000,000 while the dilution currently recommended by many authors is respectively 0.05-0.1% and 1:1,000,000. TLA without any sedation makes it possible to perform varicose vein surgery in external ambulatory surgical units outside conventional hospital centers, greatly reducing costs. |
|
Table 1. Classification of the operations and different parts of the operations (one operation could incorporate several parts). |
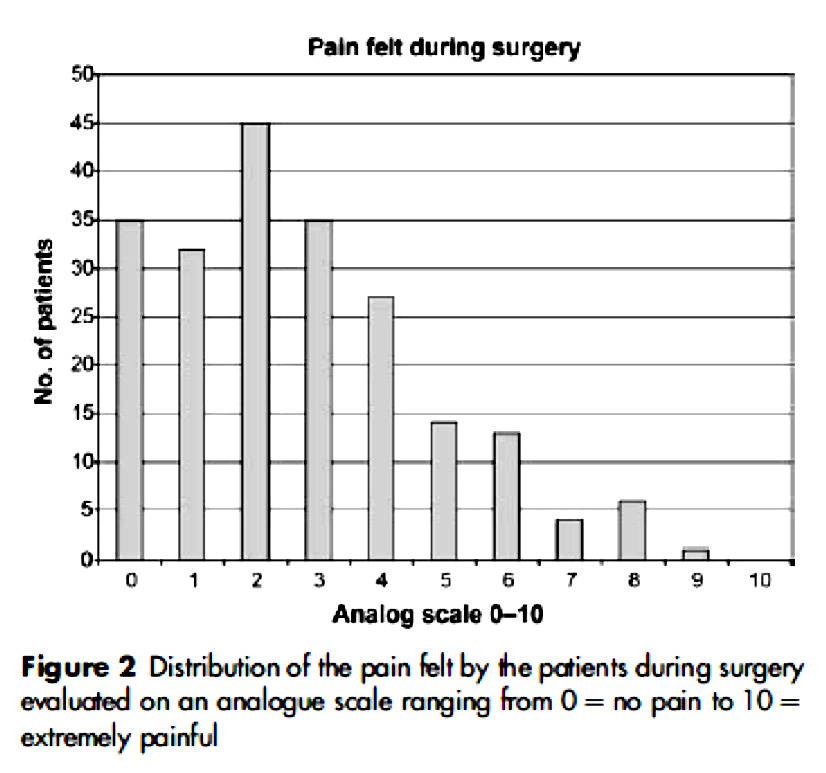 |
Figure 2. Distribution of the pain felt by the patients during surgery evaluated on an analogue scale ranging from 0 = no pain to 10 = extremely painful. |
This type of local anesthesia increases the possibilities of carrying out surgical interventions in an outpatient setting. This is of particular importance in times in which health services face serious economic difficulties. The reduction in lydocaine and epinephrine dosage when diluted in isotonic sodium bicarbonate is particularly interesting. Furthermore, when performing surgery under local anesthesia, it is well known that most of the discomfort for the patient is due to the painful infiltration procedure, presumably due to lidocaine/epinephrine acidity. Dilution with pure sodium bicarbonate instead of saline greatly reduces the infiltration pain because of the inherent production of non-ionized lidocaine that passes more easily through the cellular membranes. However, the Authors should not forget that outpatient surgery of varices under local infiltration anesthesia (without any sedation or pre-medication) was made popular worldwide during the 1960s by Robert Muller,1,2 either with ambulatory phlebectomy, or, through the work of his colleague Dr. Crossetti, with ambulatory saphenectomy. Muller’s pupils subseuently published several papers on outpatient varicose vein surgery.3 Even a European Society of Phlebectomy was created. The novel approach outlined above concerning the infiltration solution is just one more step along a road which has already been well defined. Unfortunately, this solution is often not taken into consideration, as demonstrated by the absence of any reference to the papers of Muller et al.
I agree with your two comments. This article aims to demonstrate that it is possible to perform stripping under local anesthesia without intravenous sedation. Despite the difficulty I had in finding articles in the literature about this topic, I saw this method being used in an outpatient setting by Paolo Santoro in 1986! It would have been possible to observe this same procedure even earlier in Italy and Switzerland. The aim was to show that using 1.4% sodium bicarbonate as excipient at the tumescence definitely makes things easier. We wanted to assess this feasibility in 215 consecutive cases. We did not study the level of pain level of the injections (that are completely painless) since, before using this type of tumescence, our injections for local anesthesia were already painless (lidocaine mixed at 50% with 1.4% sodium bicarbonate). In these solutions, a low concentration of sodium bicarbonate was used to neutralize lidocaîne acidity and make injections painless. It is a highly significant aspect of the procedure that surgeons who do not use lidocaïne alkalinization know nothing about.
1. Muller R. Traitement des varices par la phlébectomie ambulatoire. Phlébologie 1966;19:277-9.[PubMed]
2. Muller R, Joubert B. La phlébectomie ambulatoire. Paris: Les Editions Médicales Innothéra; 1992.
3. Ricci S, Georgiev M, Goldman M. Ambulatory phlebectomy - A practical guide for treating varicose veins. St. Louis: Mosby-Year Book Inc.; 1995.
[TOP]