Francesco Ferrara
ObjectiveJust how useful can be a study into the history of sclerotherapy is not dictated by mere curiosity but rather by the need to find a scientific model which can help develop clinical method. This means looking for an overall vision of fundamental principles and assumptions that can explain the technical choices and options offered by sclerotherapy and that can guide their development. That means defining an evolutionary rationale capable of understanding and calculating how sclerotherapeutic methods should be developed. |
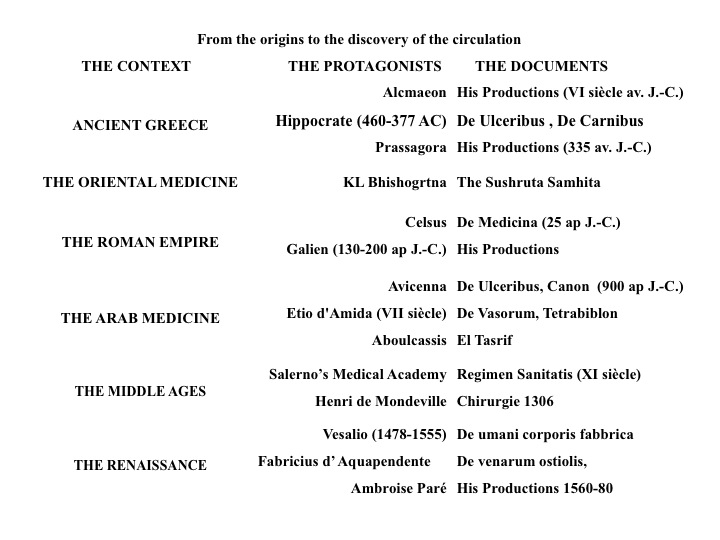
The search for a Scientific Model was made through examination and analysis of historical documents (Tables 1 and 2) according to philosophical scientific methods. This type of approach is much pertinent to the field of medicine than, for example, the philosophy of law is part of the expertise of someone who works in the field of legal science. In fact, it allows the physician to evaluate the nature of the scientific model, methods of treatment and their effects and efficacy. This process can be compared to a compass that can help us navigate between different scientific proposals. But the compass needle needs to be drawn in a specific direction and in the field of medical and scientific research it is historiography that provides the necessary magnetism. In fact, historiography is the interpretation of historical events with the aim of identifying valid reference and pertinence to current ethical and behavioral choices.
|
Table 1. From the origins to the discovery of the circulation. |
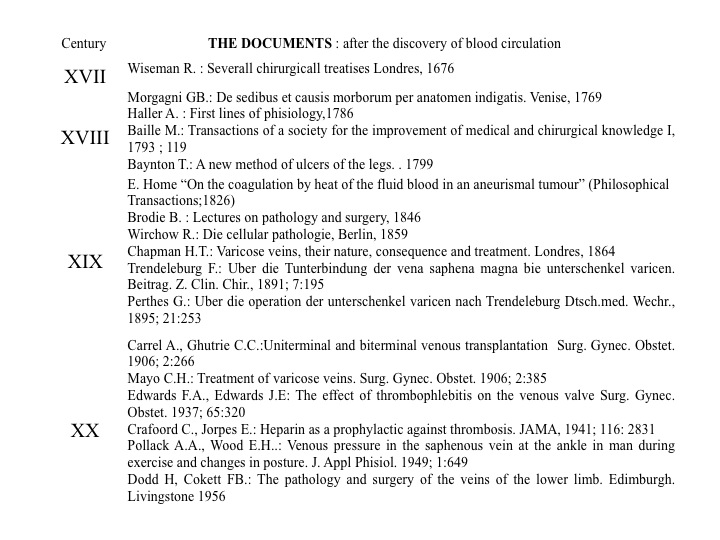 |
Table 2. The documents: after the discovery of blood circulation. |
Our question is, what type of historiographic investigation, or what method of historical analysis, should be used to validate the construction of the Scientific Model? Among the many available we have chosen the Method of the Phases of Science proposed by Thomas Samuel Kuhn (1922–1996) that has been widely used in the biomedical field. In his analysis of a historical journey/development/narrative of a technique or a scientific discovery Kuhn identified 5 phases:
Phase 0 or the pre-paradigmatic phase is that in which artistic inspiration dominates over scientific inspiration due to the obvious lack of a system of technically and scientifically accepted principles. We can call this the period of Ancient and Medieval sclerotherapy, in line with the related historical eras.
From its origins to the Surgery Congress in Lyons in 1894. The origins of the art of therapeutic veins thrombosis date from the 4th century BC and come from incidental reports. Hippocrates reports an ulcer being healed after a thrombosis, perhaps due to iatrogenic infection, in the affected vein. A similar experience was reported on a dog in 1642 by Etmüller, and in 1667, on a man by Elshortz who had made repeated attempts to use a hollow bone to cannulate a vein in order to introduce pharmacological substances. It was only in the 19th century that Hodgson (1788-1869) had the idea of suppressing the blood flow in a vein during a thrombotic event. But it was Home who, on 16th September 1825 in Chelsea Hospital, was the first to carry out a thermal percutaneous thrombosis of an aneurism by introducing a heated needle in the external iliac artery. The method was used for the first time in the field of phlebology by Palasciano at the Ospedale Incurabili in Naples in 1851. Instead of heat, he used a galvanic current delivered to the upper leg through the large saphenous vein by two crossed needles that pierced the blood vessel. The same year, Pravaz (1791-1853) in Lyons, using a syringe of his own invention, thrombosed an aneurism by injecting iron perchloride. However, the first venous sclerosing injection was performed in Paris in 1853 by Chassignac. Use of the method soon spread thanks to the efforts of the two groups in Lyons and in Paris. The principal members of the Lyons group were Valette, Petrequin, Soquet, Desgranges and Guillermand. They proposed the use of iodotanic liquid as sclerosing agent. In Italy, the leading figures in this field were Porta (1800-1875), who used chloral hydrate, and Schiassi, who in 1908 suggested the use of intraoperative sclerotherapy during venous ligation with iodinated solutions (potassium iodide). Septic and phlebotic complications were common and the Surgery Congress in Lyons in 1894 banned the use of sclerotherapy. This is a date worth remembering. Just as the fall of the Roman Empire in 476 AD signaled the end of the ancient world, so the Surgery Congress in Lyons signaled the end of the era of Ancient Sclerotherapy and opened the doors to.......
Everyone knows that the first part of the Middle Ages was dominated by the bigoted fear of imminent universal catastrophe. This is a useful analog for our discussion because it gives the idea of how, at the dawn of the 20th century, the fear of provoking pulmonary embolism and other complications was widespread. In spite of this, Delore continued to defend the use of sclerotherapy declaring, with visionary insight, that its mechanism of action was to harden the vein and not thrombose it. But a new age also began for phlebology and it was precisely in 1916 that Linser accidentally discovered that an injection of salvarsan hardened the veins without any important thrombotic element. Delore’s prophetic innovation, ignored as it was at first, became clinical evidence in those young men who were saved from the agonies of syphilis only to be sacrificed in an absurd war. They called it simply the Great War, before they were forced to number it by the wave of fanaticism and murderous fury that swept out of Germany and which, only decades later, devastated the whole of Europe. The evils that gave it birth fed the melting pot of the 1920s, followed by crisis and a degeneration of ethical values. These years did, however, see a happy return to the use of sclerotherapy thanks to the ingenious activity of Sicard (1872-1929) and his school. Already in 1920, together with Paraf, Forestier and Gaugier, Sicard used sodium carbonate as a sclerosing agent in blood vessels. He went on to perfect the technique using sodium salicylate in 1922 thanks to the assistance of other young students such as Delater, July, Filderman, Humbert and a certain Raimond Tournay, who had already stepped into the limelight in 1928 for his proposed method of thrombotic evacuation. In 1932, the Madrid Congress of the International Society of Surgery officially rehabilitated sclerotherapy. This was an unexpected and important development and it signaled the end of the dark Middle Ages.
Kuhn believed that the pre-paradigmatic phase is followed by that in which the collection of theories and methods that defined an acceptable course of conduct is articulated and called Paradigm. Continuing our comparison with historical periods, this phase can be said to correspond to the Modern Age that opens with the Renaissance. The ancient and medieval technique of sclerotherapy was, case by case, an improvised technique using subjective intuition. This differed from doctor to doctor who sometimes used contradictory approaches; some performed the injection using a tourniquet, while others banned its use, some who carried out the technique on patients with their legs raised and others with their legs hanging down, some with the patient standing, or starting with the biggest veins or those lowest down or even allowing the patient to choose which veins to intervene on first! Finally, there were some doctors who added heparin to the sclerosing agent such as Savonuzzi e Cavallini. In its Renaissance period in the 1940s, three well-defined and codified methods or paradigms (according to Kuhn) of sclerotherapy were developed. The key players in their development were Tournay in Paris (1893-1984), Karl Sigg in Basle (1912-1987) and Fegan in Dublin (1921-2007). These three methods were accepted and introduced by phlebologists everywhere with the exception of the USA. Sclerotherapy had been introduced into the US by Dixon in 1928 at the Mayo Clinic. But after 10 years of disappointing results the technique was abandoned. In fact, sclerotherapy was adopted mostly in France, Italy and Switzerland.
This was the period in which most related scientific articles were produced. This led to knowledge of the technique becoming more widespread. It was during this period that most of the sclerosing agents, many still in use today, were first introduced into clinical practice (Figure 1). Only three paradigms dominate over all the others because they reflect with precision the three fundamental classes of scientific speculation: rational, practical and critical. The rational method is typical of deductive logic as exercised by Aristotle and Cartesium. It privileges the application of a universal principle to the individual context. This was the method adopted by Tournay. In fact, it was he who raised the experience of Trendelenburg (the theory of the descending vessels) to a universal principle that proposed to use sclerosis to occlude only the saphenic reflux, thus suppressing venous hypertension and with it most of the varicosis. Sigg held a different view. He did not recognize the value of a universal principle in determining varicosis. He, therefore, adopted the inductive logic of Bacon and Galilei who used practical experience as a basis on which to develop general rules (not to the universal principles of the rationalists). Sigg preferred to suppress first of all the veins, the only practical way to guarantee that every reflux would be controlled wherever it was located. Sigg developed his assumption through simple rules that today we would call recommendations: injection in the drained vein, with an uplifted limb and immediate elastic compression. Everyone knows that the old conflict between rationalists and empiricists was only laid to rest when Kant introduced Criticism; with his I the Legislator he perceived the need to criticize the same empirically perceived faculties of reasoning as he would any piece of evidence. This teaching inspired Fegan who continued on both the principles of Trendelenburg and the rules of Sigg. He did not believe that varicose veins were the result of venous hypertension, nor did he relegate the saphenous-femoral reflux to a mere effect of the veins. He proposed sclerotherapy of the perforators and raised the turbulent flow generated by their reflux to the realms of primum movens in the pathogenesis of varicosis (ascending theory). In Paris in 1947, Tournay founded the first Phlebological Society. During the meeting of 28 February 1948, he outlined a new professional figure called the phlebologist. Whether he or she was to be considered a specialist or not, the field of interest of this new figure would be venous and circulatory diseases of the extremities. More and more meetings were organized with ever-growing numbers of people taking part. This growing interest led to the launch of the first journal, Phlebologie. As the journal became better known, the first international congresses were organized which, in turn, required the support of other societies. The first was founded in Italy in 1953 with Bassi and Comel. This was followed by other societies being formed in Belgium in 1957 with van der Molen, in Germany with Olsen, Krieg and Jaeger, in Switzerland in 1961, in Canada in 1973, in Argentina in 1975, in Japan in 1981, in the USA in 1985 and in Australia in 1993. This Normal Science period saw both successes and failures. According to Kuhn, these failures are to be considered abnormalities or events that go against the efficacy of the paradigm.
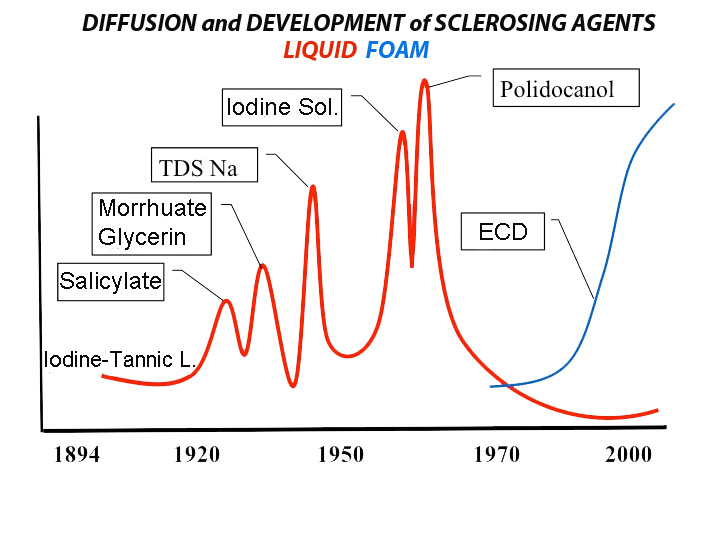 |
Figure 1. Diffusion and development of sclerosing agents. |
When the failure is particularly stubborn or obvious, the abnormality can throw into doubt techniques and methods that had been consolidated by the paradigm.
In this period, different paradigms are created. These are developed not from the results obtained from the previous theory, but only from the abandonment of pre-constituted schemes of the dominant paradigm. This is what happened with the revolutionary introduction of foam, which if we want to look for a historical comparison we can compare to the French Revolution, since this also marks the end of the Modern Age of sclerotherapy in the year 2000 and opens the new era of Contemporary sclerotherapy.
The paradigms that form part of this revolution do not share the rational foundations of the previous convalidated principles and are not, therefore, comparable even among themselves. In such a context, the choice of the new paradigm, according to Kuhn, is not supported by solid methodology. It arises rather from social and mediatic foundations that are promoted by class, power and economic interests, and is thus beyond the control of scientific societies or by the scientific community itself. In fact, when this happens, the scientific community soon stops considering themselves part of it. The societies lose their scientific value and become just simple professional corporations or, even worse, become servile fig leaves, destined to cover up the shameful occult market interests. The sequence set out by Kuhn demonstrates in synthesis a sharp backward step towards the pre-paradigmatic Phase 0. We will not allow all this to happen to our sclerotherapy! The new experiences must, therefore, be developed in consideration of the logical classes of paradigms that have already been convalidated.
Verify the efficacy of the Scientific Model and move among the different new paradigms. On its own, is the well-known greater efficacy of foam enough to convalidate the greater superiority of any technique with scleromousse, with respect to the three ancient, paradigmatic and accepted methods that use liquid? This presumed superiority is thought of as a destabilizing element in the journey undertaken by Kuhn. In our experience, we have seen that the efficacy of sclerotherapy is directly proportional to the possibility of compressing the vein. That being said, we have seen the need to use compression support with sclerotherapy of the saphenous trunks, particularly in large limbs. Therefore, a sort of compression crossectomy was introduced using a particular compression medication called Safeguard. This is applied for 3 days after the sclerosis of the saphenous trunks on the site of the saphenofemoral or popliteal junction. With this innovation, while not running the risk of adventurous physical hypotheses about the mechanism of compression which has not been convalidated by any previous experience, we can draw directly from Tournay and recognize the rational principle of not allowing the wash-out of cross reflux to destabilize the sclerosis of the trunk, obtained with our usual technique according to Sigg. This strategy (known as hippocampal sclerosis or HCS) has improved results in the use of both sclerosing liquids and foams without showing mousse to have any superior efficacy. While not questioning the undoubted theoretical superiority of foam, the destabilizing effect of its introduction into therapeutic practice has been normalized by the management of the research carried out throughout the evolutionary phases of the Scientific Model. In fact, this requires the transition from the revolution in Phase 5 (Extraordinary Science) to Phase 1 (Ordinary Science) without falling back into the dark mists of Phase 0 (pre-paradigmatic).
We cannot propose a technique (with or without the support of evidence-based medicine or EBM, and with or without striking results) taken out of the context of a logic that can be defined with a Scientific Model. Its use would be desirable in every aspect of the scientific evolution of sclerotherapy, but above all in the sector that has fallen most behind, that of pharmacological research. It is here that the lack of a Scientific Method has been felt most. It is enough for us to look carefully at the graph presented in Figure 1. The introduction on the market of sclerosing agents currently in use dates from the 1940s-1960s. This means that we are still stuck back in the Renaissance!
1. Ferrara F. Sclérothérapie: ma méthode. Angéiologie 2010;62:78-82.
2. Ferrara F. Histoire de la phlébologie - Rassegna monografica. Phlébologie 2008;61:119-24.[Abstract]
3. Kuhn TS. The road since structure: philosophical essays, 1970-93. Chicago: University of Chicago Press, 2000.
4. Genovese G, Tori A, Donadi GC. Flebologia ieri ed oggi. Milano: Nuove Edizioni; 1994.
5. Kuhn,TS. The function of dogma in scientific research. pp. 347-69. In: A.C. Crombie (ed.). Scientific change (Symposium on the History of Science, University of Oxford, 9–15 July 1961). New York and London: Basic Books and Heineman; 1963.
6. Kuhn TS. The structure of scientific revolutions. Chicago: University of Chicago Press; 1962.
[TOP]