a Field Epidemiology Training Program, Epidemiology Bureau, Department of Health, Sta Cruz, Manila, Philippines.
b Department of Health, Sta Cruz, Manila, Philippines.
Correspondence to Julius Erving Ballera (email: jerving30@gmail.com).
To cite this article:
Ballera JE et al. Risk factors from a chikungunya fever outbreak in Laguna, Philippines, 2012. Western Pacific Surveillance and Response Journal, 2015, 6(3). doi:10.5365/wpsar.2015.6.1.006
Background: In July 2012, the Philippines National Epidemiology Center received a report of a suspected chikungunya fever outbreak in San Pablo City, Laguna Province, the first chikungunya cases reported from the city since surveillance started in 2007. We conducted an outbreak investigation to identify risk factors associated with chikungunya.
Methods: A case was defined as any resident of Concepcion Village in San Pablo City who had fever of at least two days duration and either joint pains or rash between 23 June and 6 August 2012. Cases were ascertained by conducting house-to-house canvassing and medical records review. An unmatched case-control study was conducted and analysed using a multivariate logistic regression. An environmental investigation was conducted by observing water and sanitation practices, and 100 households were surveyed to determine House and Breteau Indices. Human serum samples were collected for confirmation for chikungunya IgM through enzyme-linked immunosorbent assay.
Results: There were 98 cases identified. Multivariate analysis revealed that having a chikungunya case in the household (adjusted odds ratio [aOR]: 6.2; 95% confidence interval [CI]: 3.0–12.9) and disposing of garbage haphazardly (aOR: 2.7; 95% CI: 1.4–5.4) were associated with illness. House and Breteau Indices were 27% and 28%, respectively. Fifty-eight of 84 (69%) serum samples were positive for chikungunya IgM.
Conclusion: It was not surprising that having a chikungunya case in a household was associated with illness in this outbreak. However, haphazard garbage disposal is not an established risk factor for the disease, although this could be linked to increased breeding sites for mosquitoes.
Chikungunya fever is a viral illness caused by an arbovirus transmitted by the Aedes mosquito. The disease was first documented in an outbreak in United Republic of Tanzania (1952); the name was derived from the Makonde dialect and means “that which bends up”, indicating the physical appearance of a patient with severe joint pains.1
Chikungunya is an emerging vector-borne disease of high public health significance in the South-East Asia Region and has been reported from South and East Africa, South Asia and South-East Asia. In Asia, outbreaks have been reported in India, Indonesia, Maldives, Myanmar, Sri Lanka and Thailand.1
In the Philippines, the first chikungunya cases were reported in March 1968 in Amlan, Negros Oriental, affecting 698 individuals.2 The first outbreak investigation was conducted in June 1996 in Indang, Cavite, where a total of 151 suspected cases were identified.3 The first laboratory-confirmed outbreaks occurred in Davao City and Cagayan de Oro City in 2011.4
In July 2012, the Regional Office of the Philippines Department of Health for Region 4A reported a suspected chikungunya outbreak in San Pablo City, Laguna Province to the Philippines Event-based Surveillance and Response Unit of the National Epidemiology Center. These were the first chikungunya cases reported from the city since the establishment of the disease surveillance system in 2007. A team from the Philippines Field Epidemiology Training Program (FETP) was deployed to conduct an outbreak investigation to identify risk factors associated with chikungunya.
A case was defined as a previously well resident of Concepcion Village, San Pablo City, Laguna Province who had fever of at least two days duration and either joint pains or rash between 23 June and 6 August 2012. We reviewed medical records at the city health office and hospitals and a line list of cases was developed. House-to-house case finding was also conducted in the affected village.
An unmatched case-control study with a planned 1:1 ratio of cases to controls was conducted. Not all cases were included due to logistical barriers. For convenience, a control was defined as any well individual residing in the same or nearest household of a case with a negative specimen for chikungunya IgM.
A standard questionnaire which included data on demographic profiles and sanitation practices was administered to all cases and controls. All data were entered and analysed using Epi Info version 3.5.4. We calculated odds ratios (OR) and confidence intervals (CI) in bivariate analysis with significant risk factors (P < 0.05) included in a multivariate logistic regression using a forward stepwise procedure.
Environmental investigation was conducted through observing water and sanitation practices and inspecting for potential breeding sites of mosquitoes at Concepcion Village. In subvillages 3 and 4, 100 households were randomly selected for calculation of the House Index (percentage of houses infested with larvae and/or pupae) and Breteau Index (number of positive containers per 100 houses inspected). These were then compared with the goals of the Philippines National Dengue Prevention and Control Program of < 5% and 20%, respectively.5 On-site entomologists determined mosquito larvae species.
Human serum samples collected from both cases and controls were sent to the Research Institute for Tropical Medicine in Muntinlupa City, Philippines for laboratory confirmation of chikungunya IgM by enzyme-linked immunosorbent assay (ELISA) (NovaTec, Waldstrasse, Dietzenbach, Germany).
Ethics clearance was not required as this investigation was part of an emergency response to an outbreak.
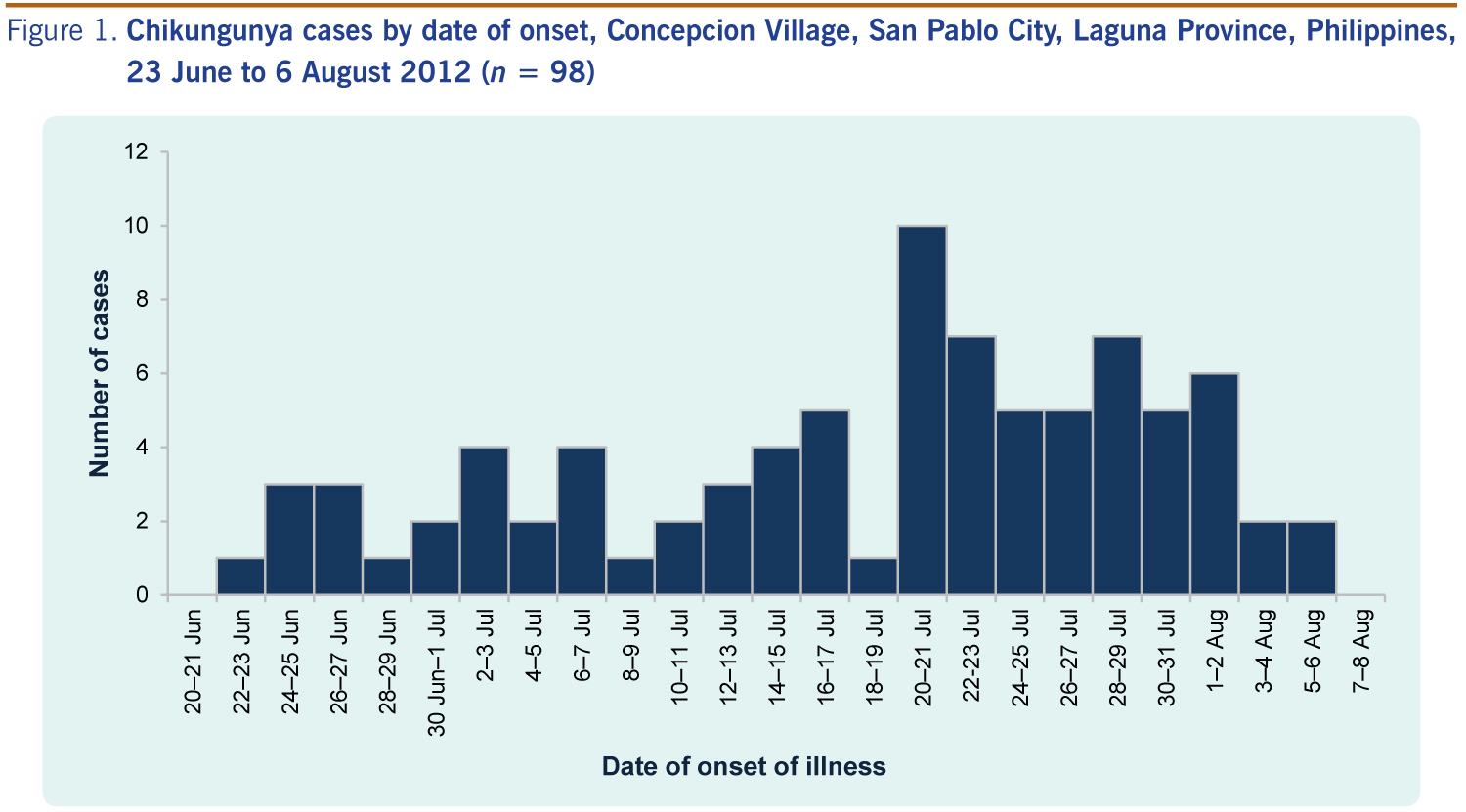
Ninety-eight cases were identified with the first case reported on 23 June and a peak in the number of reported cases occurring on 20 to 21 July (Figure 1). One (1%) case was hospitalized. No deaths were reported. Age of cases ranged from five months to 83 years (median: 27 years) and 54 (55%) were females. The most affected age group was the 11–20 year olds with 26 cases. All cases were from subvillages 3 and 4 of Concepcion Village with an overall attack rate for Concepcion Village of 1.2% (population: 7881). Aside from fever, cases also manifested with rash (88%), joint pains (85%), headache (61%) and cough (23%).
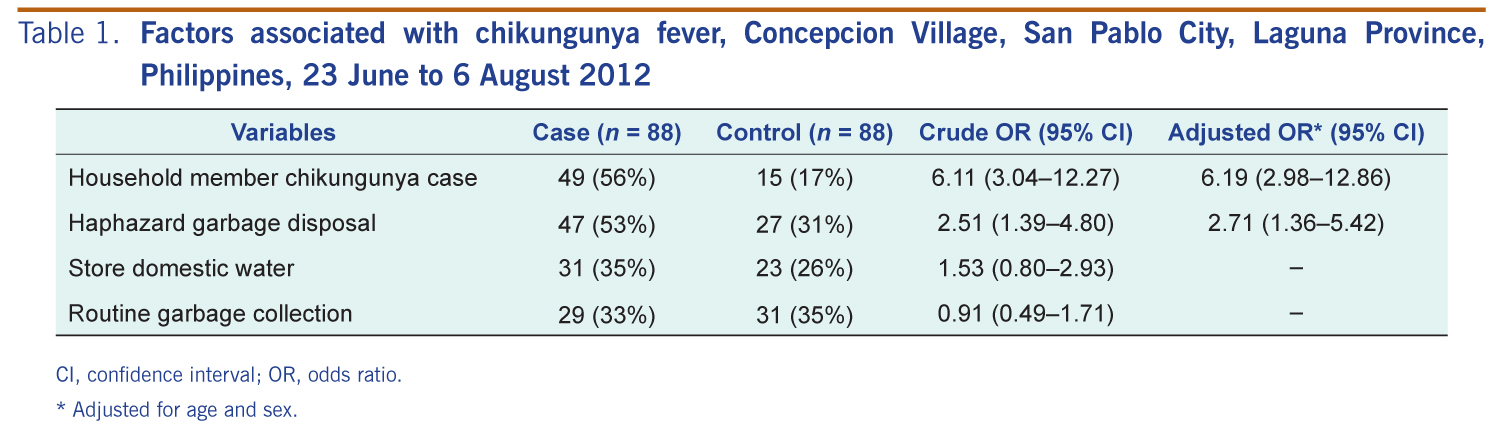
There were 88 cases and 88 controls included in the study. Both univariate and multivariate analyses showed that the odds of cases having another sick household member was six times higher than for controls (adjusted OR [aOR] 6.2; 95% CI: 3.0–12.9) and was two times higher for disposing of garbage haphazardly (aOR: 2.7; 95% CI: 1.4–5.4; Table 1).
CI, confidence interval; OR, odds ratio.
* Adjusted for age and sex.
The village is supplied by a municipal water system. However, there was no continuous water supply and households commonly stored water. We routinely observed uncovered water containers. A clustering of cases was observed near the irrigation canal. Not all households had routine garbage collection. We observed residents disposing of their trash haphazardly in a nearby irrigation canal and in backyards. Discarded coconut shells and other potential vessels for mosquito breeding were observed among garbage.
House and Breteau Indices were 27% and 28, respectively, and both were above the national standards of < 5% and < 20%.5 These high indices indicates the abundance of breeding habitats for Aedes mosquitoes and also signifies that the place is sensitive and vulnerable to disease transmission. Seventy-nine per cent of all larvae identified were Aedes aegypti and 21% were Aedes albopictus.
Of the 84 cases tested, 58 (69%) serum samples were positive for chikungunya IgM by ELISA.
A chikungunya fever outbreak occurred in Concepcion Village, San Pablo City, Laguna Province from 23 June to 6 August 2012. The outbreak was confirmed by laboratory detection of chikungunya IgM from human serum. The probable vectors identified were Aedes aegypti and Aedes albopictus mosquitoes, known carriers of the virus.6 During the environmental investigation, we observed multiple breeding sites in the irrigation canal and backyards. Entomological survey showed high larval indices in the outbreak subvillages. Other outbreak investigations conducted by FETP fellows from the Department of Health, Philippines have found similarly high larval indices in their own settings.4
Having a chikungunya case in the household was a strong risk factor for acquiring the disease in this outbreak. This finding is consistent with results from a large-scale survey recently conducted in Haiti.7 The World Health Organization recommends that any household member suspected of chikungunya fever should rest under bed nets during the viremic phase to limit the spread of infection.6
Haphazard garbage disposal was found to be another risk factor. It was observed that this garbage was disrupting the free-flow of the irrigation canal which would increase breeding sites within the canal and also provided more containers for pooling of water where mosquitoes can breed. Haphazard garbage disposal has been shown to be a risk in other vector-borne disease outbreak investigations,8 most likely as it increases breeding sites for mosquitoes.
In this study, we limited our house-to-house case finding to two subvillages. It is possible that we may have missed cases from nearby subvillages. Using a clinical case definition may have resulted in misclassification, especially as almost a third of cases included in the analytic study were negative for chikungunya IgM. Also, the method employed in choosing controls limited the capacity to test place-related risk factors such as proximity to the canal.
Although chikungunya has a relatively low case fatality rate, attack rates can be high. Persistent joint pains can lead to disability and reduction of productivity,9 therefore the public health burden of chikungunya is significant. Upon the recommendation of the investigation team, the community response to the outbreak included establishing routine garbage collection throughout the affected subvillages and weekly monitoring of larval indices. We recommend that investigators of future chikungunya outbreaks consider evaluating haphazard garbage disposal as a risk factor for increased breeding sites for mosquitoes.
None declared.
None.
{kind=link}
{kind=link}